




Female Athlete Triad - Symptoms and Treatment
Female Athlete Triad
- This is a condition found in active females
- It is composed of three components:
- Low energy availability with or without an eating disorder
- Menstrual dysfunction
- Decreased bone mineral density (BMD)
- For each component there is a spectrum of severity from normal to most severe
- Women may be affected by one or all of the components of the triad simultaneously
- It is therefore important that any female athlete presenting with any one feature of the three components to be screened for all three
- The prevalence of having all three parts of the triad at the same time is not common ~1%
- Prevalence of any two is ~20%
- Prevalence of just one is ~40%
- Women who are involved primarily in sports that focus on weight or aesthetics e.g. running or ballet are more at risk
- The approach to treatment is challenging due to the complex nature and interconnection of the three factors
- Treatment is optimised through a multidisciplinary approach:
- Physician
- Psychologist or psychiatrist
- Dietician
- Physiotherapist
- Coach:
- They focus on a team success through team skills and strategies
- Athletic trainer:
- They focus on optimising fitness and injury prevention for an individual athlete
- Family members:
- They are key to providing continued support and encouragement
- Patient:
- Patient education is key to helping them understand their condition, the potential consequences and the benefits of receiving treatment
- Patient should have a thorough and holistic examination and laboratory tests to assess:
- Which organs have been affected
- Bone mineral density though DEXA scan as they are at risk of earlier osteoporosis
- Nutrition
- Menstrual dysfunction
- Psychological and behavioural health
- The aim of treatment is to:
- Consume sufficient calories to provide a positive energy balance:
- This is the first and most important step
- Resumption of menses:
- Nonpharmacological options are usually first choice
- Medication tends to be reserved for those with oestrogen deficiency or infertility
- Improve bone mineral density:
- It is essential for health care professionals, coaches, personal trainers and nutritionists dealing with female athletes to be aware of the Female Athlete Triad as the consequences can be severe
- The best approach is education and prevention of this condition with regular screening of athletes for concerning behaviours and signs and symptoms of the triad
- Early detection and appropriate prompt intervention is required once diagnosed
- Bone is highly responsive to loading activities such as impact and resistance training:
- However, they need to be tailored to the patient and the severity of loss of bone mass and should be progressed gradually
- Doing high impact activities from the outset in the presence of grossly weakened bones can lead to stress fractures
Low energy availability
- Energy availability is simply:
- Energy intake in the form of calories consumed minus
- Energy that is used up through:
- Exercise
- Activities of daily living:
- These are activities of self-care e.g. feeding, cleaning, dressing
- Normal bodily functions:
- Cellular maintenance:
- Body has 37 trillion cells!!!
- Takes a bit of energy looking after all of them
- Cells replicate and divide to replace dead or damaged cells
- Most cells in the body can do this
- Heart muscle cells and nerve cells are not able to and so what you are born with is all that you have and once they die off there is no replacement
- Thermoregulation:
- Maintaining body core internal temperature within a small range of 37 degrees Celsius
- Reproduction:
- Energy spent through the menstrual cycle
- Low energy availability can be due to a host of factors:
- It can occur without an eating disorder
- Unintentional:
- Athlete is unaware how many calories are required to offset what has been consumed
- Intentional:
- Conscious decision to reduce calorie consumption:
- This can be part of an eating disorder involving:
- Restricted eating
- Elimination of specific food groups
- Fasting
- Skipping meals
- Diet pills
- Laxatives
- Diuretics
- Binge eating followed by intentional vomiting
- Excessive exercise:
- The single most important factor associated with suicidal behaviour in females with an eating disorder is exercising excessively
- When there is negative energy balance i.e. caloric intake is less than the body’s energy expenditure, then the body will reduce the amount of energy directed to maintain bodily functions such as cellular maintenance, thermoregulation and reproduction
- Irrespective of when the eating disorder presents itself, the poor eating habits and behaviours are formed during adolescence
- The prevalence of eating disorders in adolescent and young female athletes is ~30%
- High school athletes with eating disorders are twice as likely to sustain a musculoskeletal injury


Consequences of someone with an eating disorder
- Effect of poor diet:
- Significant and rapid weight loss not explained by another illness
- Lack of expected weight gain during puberty
- Feeling full after only a small amount of food
- Fatigue
- Gastrointestinal irregularity:
- Constipation
- Diarrhoea
- Mental health issues:
- Chest pain with or without palpitations
- Low self-esteem
- Depression
- Anxiety
- Compulsive behaviour
- Sleep disturbance
- Gynaecological impact:
- Delayed onset of menstruation
- Cessation of menstruation
- Infertility
- Impact on renal function:
- Poor hydration leads to electrolyte imbalance
- Increased risk of cramps
- Acute kidney failure
- Chronic kidney failure
- Musculoskeletal problems:
- Stress fracture
- Delayed healing following an injury
- Socioeconomic impact:
- Lower academic achievement
- Lower socioeconomic achievement during early adulthood and later on
Menstrual Dysfunction
- This like the other two components can be at any part of a spectrum of severity ranging from:
- Eumenorrhoea (normal menses)
- Primary amenorrhoea:
- Delayed onset of menses beyond 15 years of age
- Secondary amenorrhoea:
- Cessation of menstruation for 3 consecutive months in a female who has already started menstruating
- Oligomenorrhoea:
- Regular menstrual cycles but wider apart (>35 days)
- Menstrual irregularity is:
- Very common (~90%) within the first two years of menarche (onset of menstruation) and so caution should be used before diagnosing menstrual dysfunction in this age group
- Menstrual dysfunction is highest among lean and aesthetic athletes:
- Gymnastics, diving, dancers, cheerleaders
- Can lead to infertility:
- Women with amenorrhoea are infertile as they do not produce ovarian follicles or ovulate
Low bone mineral density (BMD)
- BMD in the female triad is along the complete spectrum from normal bone density to osteopaenia and osteoporosis
- The prevalence of osteopenia is ~35% in female athletes and osteoporosis ~7%
- In comparison the prevalence of both is 12% and 2% in the general population thus showing a 3 times higher risk for female athletes
- A DEXA scan is required to assess BMD (further information can be found here)
- The T-scores which are typically used for osteoporosis in post-menopausal women are not suitable for young people and so the Z-scores are preferred as these compare individuals to people of the same age, sex and ethnicity (unlike T-scores which compare the value to a healthy 30 year old individual)
- A Z-score in adolescent or premenopausal females that is below -2.0 e.g. -2.1 or -3.0 (which is worse than -2.1) is termed low BMD for chronological age
- Further information for causes of low BMD and how to optimise bone density throughout life can be found in the article How to Best Invest in your Bones
- Athletes whose sport involves mainly weightbearing activities are known to have higher BMD and because of this the American College of Sports Medicine defines:
- Osteopaenia in an athlete to be a Z-score between -1 and -2 together with risk factors for fracture such as amenorrhoea, reduced energy availability, and history of a stress fracture
- Osteoporosis in an athlete to be a Z-score less than -2.0 (e.g. -2.1) with risk factors for fracture
- The greatest amount of bone accrual occurs during puberty and in girls between 11-14 years
- 25% of the gain in bone mass occurs within 2 years of menarche
- 92% of the gain occurs by 18 years
- 99% of the gain occurs by 26 years
- Exercise can help improve gain in bone mass by 5% in children
- Amenorrhoeic athletes who play the same sport as eumenorrhoeic athletes, will have lower BMD:
- Studies have shown as much as 10-20% reduced lumbar spine BMD in amenorrhoeic athletes compared to eumenorrhoeic
- This shows that the beneficial effect of exercise on BMD is much less than the detrimental effect of amenorrhoea which should raise alarm bells in adolescent female
- If amenorrhoea continues and goes untreated 2-3% of bone mass will be lost each year
Complications of Female Athlete Triad
- Infertility
- Raised bad form of cholesterol (Low Density Lipoprotein)
- Increased risk of cardiovascular disease
- Reduced immunity
- Stress fractures:
- 2-4 times more likely than eumenorrhoeic females
- Most frequent site is tibia (~50% of stress fractures)
- Lower peak bone mass achievement than eumenorrhoeic females:
- This puts them at higher risk of developing osteoporosis
- Depending on the duration of the triad, measures taken to improve BMD and time to recovery, BMD may not catch up to the expected BMD for someone of the same age as the patient
- Nutritional deficit can include:
- Deficiency in essential amino and fatty acids can lead to reduced ability to repair damaged tissue, build muscle mass and recover from injury
- Low energy availability can lead to:
- Depression
- Low self-esteem
- Anxiety disorders
- Increased risk of suicide and earlier death associated with the more severe eating disorders such as anorexia nervosa and bulimia
- Low energy supply can adversely affect numerous systems:
- Gastrointestinal
- Metabolic
- Endocrine
- Immunological
Further helpful information can be found here on:

Introduction De Quervain’s tenosynovitis (also called De Quervain’s tendinosis) is a painful condition of two tendons at the level of the wrist on the side of the thumb It’s a repetitive strain injury due to overuse of two tendons used to move the thumb away from the other fingers

Introduction Cubital Tunnel Syndrome occurs when the ulnar nerve is compressed within a tunnel on the inner (medial) side of the elbow just behind the bony prominence of the inner aspect of the elbow called the medial epicondyle Cubital Tunnel Syndrome is the second most common cause of peripheral nerve compression: The most common one being carpal tunnel syndrome (compression of the median nerve at the wrist) The ulnar nerve is one of the three main nerves of the upper limb: The other two nerves of the upper limb are the median nerve and the radial nerve The ulnar nerve travels from the neck past the elbow and wrist and into the hand: Along the way it travels past some narrow areas where it can be constricted and cause symptoms for the patient The most common site of ulnar nerve compression is in the cubital tunnel at the elbow The second most common site is in Guyon’s canal in the hand When someone accidentally hits the inner side of the elbow (often termed hitting the funny bone) they get a sharp tingling sensation on the inner side of the elbow and forearm: This occurs because the ulnar nerve was hit at the site of the cubital tunnel where the nerve is close to the skin surface and therefore easily injured from outside forces
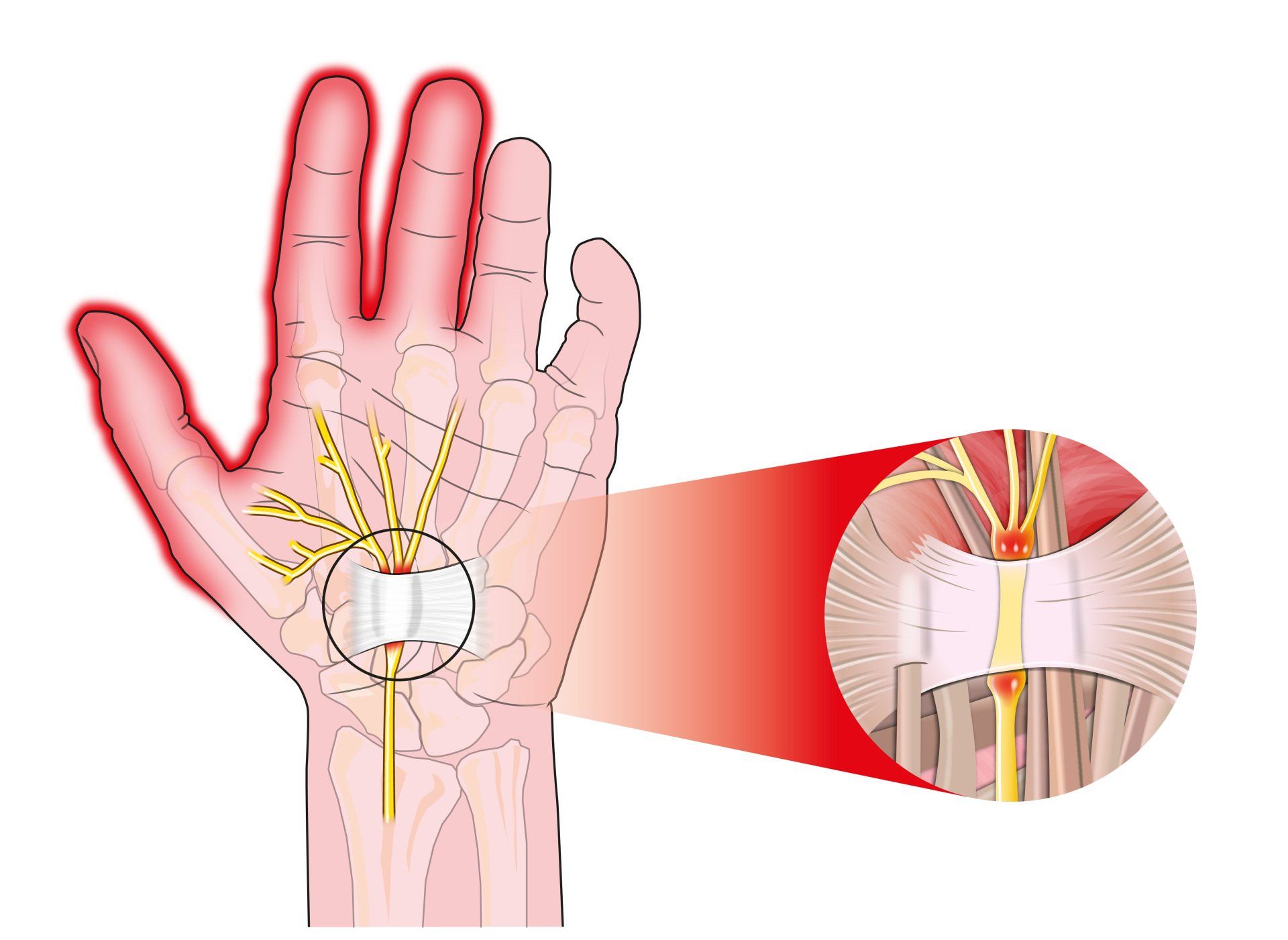
Introduction Carpal tunnel syndrome is a common condition that causes numbness, tingling and weakness in the hand specifically affecting the thumb, index and middle fingers: The little and ring fingers are not affected as they are supplied by another nerve called the ulnar nerve It is the commonest cause of peripheral nerve entrapment It is caused by compression of the median nerve as it passes from the forearm into the hand through a passage called carpal (i.e. wrist) tunnel The median nerve is one of three main nerves that supply the upper limb: The other two nerves are the ulnar nerve and the radial nerve
Introduction Tennis elbow (also known as lateral epicondylitis) is an overuse injury of the forearm tendons that originate over the lateral epicondyle of the humerus (bony prominence on the outside of the elbow) and act to bring the wrist backward away from the palm Whilst tennis players are particular prone to this condition it does not occur exclusively to them

Introduction This term is also known as repetitive motion or stress injury and occurs as a result of carrying out the same motion repeatedly over time causing injury to muscles and tendons It is associated with repetitive tasks, sustained or awkward position, forceful exertion, vibration or compressive forces It can affect almost any joint in the body Most commonly affected areas are hands, wrists, shoulders and neck It is thought to affect 5-10% of the general population but can be as high as 20-40% in specific working populations

The most common injuries in sailing, are in the waist (45%), knees (30%) and shoulders (20%). Causes of sailing injuries, windsurfing injuries, sprain or ruptured knee ligament. Injury prevention, protective clothing to avoid injuries in sailing.

Injuries such as concussion, anterior cruciate ligament injury, anterior gonalgia, fatigue fracture, tibial periostitis, ankle sprain, rotator cuff injury should be avoided for women to exercise.

Women have a 50% higher risk of developing pathologies when running and exercising. Prevention of Sport Injuries.

What is the function of vitamin D - The benefits of vitamin D, what amount of vitamin D should I take, which foods are high in vitamin D, risks of vitamin D deficiency, the role of the sun, osteoporosis, causes, symptoms.
Read all about osteoporosis, what causes it, frequency in women and men, fracture prevention, diagnosis and treatment.